
Sci-Fi Today: Chemogenetics
Changing the brain, but for science!

Sometimes when we think about our behaviors, our selves, and the choices we make, it’s hard to fully understand the neurological underpinnings of that. It’s hard to wrap our minds around the idea that when something frightens you, makes you nervous, makes you happy, sad, angry, and then you act on these emotions, our brains are in action.
Think about it! When you perceive the outside world, you are perceiving it because your senses are able to deliver the information through the proper pathways into the brain. Then you’re not sensing, you’re perceiving. Then we act on those perceptions mechanically, and the process continues in the reverse. Simply put, at the end of all things is our brains acting out the drama that is us. Kinda cool, right? But what if we changed how we received that input? What does that even mean? What does that mean about who we are, how we act, or what it even means to sense, perceive, and behave? Fortunately, we don’t have to think too hard about that just yet, but… maybe it wouldn’t hurt to start.
Hey everyone! Welcome back to Sci-Fi Today! A little series where I give myself an excuse to talk about some of my favorite research methods, how they work in practice, and how they could make your sci-fi just a little more interesting! Today, we’re looking at something called Chemogenetics. There is some crossover between methods like chemogenetics and optogenetics, so if you are interested in optogenetics, I highly recommend you have a look at the always wonderful Rachel LaDue’s page where I did a guest post last year talking about optogenetics and how it could work for one of her fantastic serial characters here.
For those of you new around these parts, I’m L.L. Ford, your resident neuroscientist and fiction writer! Since the last Sci-Fi Today I’ve also become a doctor, so for the sake of the science, Dr. Ford is in for this post! But that’s not important right now. For now, let’s talk about chemogenetics! Then, I want to get into a little bit of ethics, because sciences like this are… well, in practice, they can be a little freaky. For the sake of sharing my sources, my primary source for this is a fantastic review paper called ‘The use of chemogenetics in behavioural neuroscience: receptor variants, targeting approaches and caveats’ which I will link below. Let’s hop into it!
The Science
Something I want to talk about right from the start is that chemogenetics is an extremely complicated topic. Don’t worry, I’ll do my best to do it justice while still making sense, but if at any point I entirely lose the plot or things start to not make sense, don’t hesitate to reach out and ask questions or get clarifications! This stuff is intense, and while very cool, it is also very confusing. I will also note that since this is a complex topic, there’s a lot of different concepts, ways to make it work, and different methods that have different significant uses. It’s all very cool, but there’s a lot more to dig into than I can here. I will be using a specific paper as my primary source when discussing this here, and I’m also linking that here, because I encourage you to check it out! It is a really cool paper, and they actually get into a little speculation on their own about how they think this can work with humans, so please do have a look at my sources (links are at the bottom).
So, let’s talk basics. What is chemogenetics doing? At its core, chemogenetics is an invasive brain surgery that attempts to alter the number of receptors in one region, therefore altering how many neurotransmitters are being deposited by another region (if the neuroscience concepts here are a little confusing, I encourage you to check out my sci-fi today discussing neurons!). In many cases, rather than altering just one region, you will make it so that the ligand that would activate this change would only come from another region of the brain. This would be done by injecting one brain region with drug that alters receptors (we’ll get to that later) and another region connected to that region with the ligand that activates this change. In a research setting, this is extremely helpful because then we can control for only connections between one part of the brain and another. If we didn’t do this, one brain region could end up being way over active in a lot of different ways, and contrary to what many people believe, one region of the brain can have nuanced, context-dependent functions that can change depending solely on what sort of input they’re receiving and from where that input is coming from!
Let’s look at a couple of quick examples of different approaches to chemogenetics! And I encourage you to circle back to this image later after we went over more details so you can better understand it too!
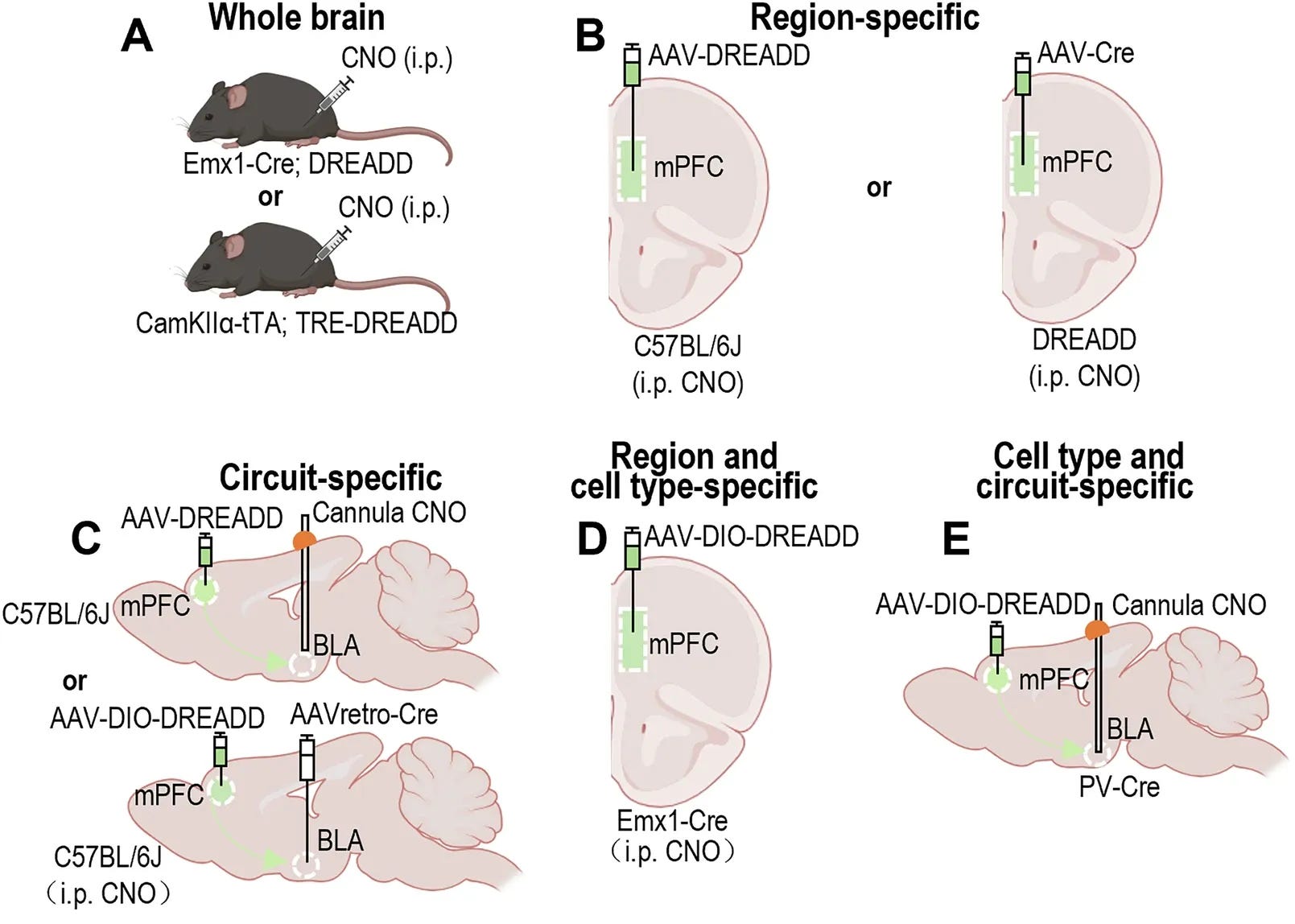
Let’s consider some more things here. The Amygdala is an extremely significant part of the brain, but it also has A TON of connections. What if we wanted to target a specific part of the amygdala’s connections? Well, we’d need to identify a subregion - I’m partial to the basolateral amygdala (BLA) - then we would need to figure out a region that’s connected to it. For the sake of this, let’s say the medial prefrontal cortex (mPFC) given that the above figure uses it as well.
Okay, so the BLA receives signals from the mPFC, right? Well, we can’t necessarily increase the number of projections without neurogenesis (Note: While it was believed for a long time that neurogenesis isn’t possible, it is definitely possible, but under very specific circumstances, and very specific regions. That’s a discussion for a different day though.), but we could alter the neurons already there. What do I mean by altering what’s already there? Enter designer drugs.
DREADDs (Designer Receptors Exclusively Activated by Designer Drugs) sound a little odd, but I’m sure many of you recognize designer drugs. Before I became a neuroscientist, I thought the concept of designer drugs was cool, but I didn’t really understand what it meant. DREADDs are a great example of what we can do with designer drugs. In this case, what we do is we can inject a drug that alters a neuron on the molecular level, basically adding designer receptors into a specific region of the brain. But here’s the important thing: We don’t want to just create receptors on a bunch of cells. Then you can’t control what’s inputting there. Instead, what if these receptors could be activated by designer drugs that we can manually put in ourselves? From the figure above, you may see a lot of mentions of CNO. CNO would be our designer drug that would then activate these designer receptors!
Think of it this way: one region of the brain can be involved in many different functions. We don’t want those other functions to be impacted by altering the receptors on these cells, but if we already know what a connection between two regions might do, then we can target the receptors impacted by another group of cells. But how?
There are two primary components to keep in mind during this process (trust me, there’s more than two, but we’re keeping it as simple as possible for now!). We have our receptors and our ligands. These are both things that we as the scientists are adding into the system. We do this through stereotaxic injections or system-wide administration if you’re not worried about targeting a specific part of the brain. Stereotaxic injections are extremely precise surgical injections into a brain. I personally have performed quite a few of these and it is a very time consuming and precise practice that is extremely rewarding when you do it right and beyond frustrating when you do it wrong. Why? Sometimes you don’t know if it worked until weeks later. Literally 2-3 weeks later.
I want to point out that saying we have a ligand and receptor - while true - is very reductive. I want to be careful not to be so reductive that I’m no longer stating facts, so let me clarify a couple small things. When you inject a DREADD into the system, you need for it to actually be able to spread properly. DREADDs can’t do this on their own, so we need viral vectors with them. There are a ton of viral vectors you can use, and it can depend on what specifically you’re doing. The kind I’m most familiar with (both through literature and lab assays) is the Adeno Associated Virus (AAV). There’s a bunch of different types of AAVs that can do all sorts of things, but we don’t need to worry about that right now.
Another thing we may have to take into account is the promoter which acts as our ligand. A promoter will be administered during and after our DREADD has been administered to manipulate the impacted region and ‘promote’ our receptors to stay active. It is not the same thing, but I always thought of it sort of as taking a medicine. Yes, everything is there and ready to go, but without your promoter to get everything working again, nothing is going to happen. There’s a few different promoters people use, but the one I most commonly see (the one used in my lab from grad school, and mentioned above) is CNO (Clozapine N-Oxide). CNO is a tricky one because it can have impacts on behavior aside from our intended changes, but it is fairly popular even today.
Okay, so now we have that out of the way, let’s work through what’s really happening. So, we put our mouse (we’ll say mouse for now) to sleep and we’re all prepped for surgery. Let’s revisit our connection between the mPFC and the BLA. We have our coordinates for our target region all ready to go, so we inject our DREADD directly into the mPFC. This will then travel along the established circuit and to the BLA, but we need time for it to travel and for our mouse to recover. That’s the surgery done. Now what? Now we need to wait a few weeks.
Once there, we can inject our CNO directly into the BLA through a cannula that we already placed. Mind you, we would need DREADDS specifically designed to receive our promoter. Later down the line, you’re going to want to reintroduce your promoter, I’ve heard of people doing oral introductions of promoters or even needle injections into the blood stream, but if you want to ensure maximum effect, you’ll want to put a cannula in place over your presynaptic region (the mPFC) so you can later readminister your promoter without having to do a whole new surgery again.
Once all the difficult and stressful surgeries are done, you can do all kinds of tests, but let’s say for the sake of simplicity, we’re trying to figure out some sort of behavior change. Depending on what area you were testing and what your hypothesis might be would determine what sort of tests you’d be running. Now, I’m not a behavioral neuroscientist BUT if I were looking at connections between the mPFC and BLA, I think I’d want to run a couple of social tests. Maybe a home cage intruder test, three-chamber sociability and social novelty tests, and maybe some general anxiety/stress tests like an open field test and an elevated plus maze. I would mostly do those general tests so we can see if changes in social behavior are changes to social stress and anxiety only or if it is generally impacting stress and anxiety. That’s an important nuance! And for those of you who work in the sciences, you may be thinking ‘well, we need a control then.’ And yes we do!
If we were being extra rigorous, I’d say we should have a control group that received only saline stereotaxic injections instead of CNO but still had their DREADDs, as well as a group that had no injections of any sort. We may also want a CNO injection with no DREADDs because as I said, CNO does have some established impacts on behavior! In a perfect world, we’d want those controls to be broadly the same, but we would also expect the trauma of surgery to have some long-term impacts as well as the CNO.
So, I’ve generally explained how this works, and how it would be used scientifically but why would we even go through all this trouble anyway? Well, there are a few reasons. One such reason is that by messing around with connections between two brain regions, we can better understand what the targeted circuitry even does.
We could also be doing this because we know what’s associated with those regions, but we want to see how it may be different under different genetic changes. For example, we know there are differences in connectivity in a lot of neurodevelopmental disorders, so maybe we could target these regions to figure out if altering them changes behavior. Does altering the behavior pull them further away from neurotypical or will there be some sort of baseline? This can help us better understand how different genetic and environmental changes may be impacting part of the brain, but is it a treatment? Should it even be considered as treatment? I’m not so sure.
Now, this is all really interesting to think about in a genetic animal model, but what about humans? Well… I take issue with this, and I think we need to ask a few questions about that. Why would we do this to a human? Is it worth it to do it to a human? And would this actually be helping a human? Let’s talk a little about ethics.
The Ethics
I’ve always loved that line from Jurassic Park - how does it go? “You spent so much time wondering if you could, you never stopped to ask if you should.” You get the idea (I also love to misquote it apparently because I’m refusing to look up the exact wording). It’s a good question though! So, we can use viral injections, genetic alterations, and light manipulations to change the way different parts of the brain operate, right? But should we?
As a scientist, for the sake of uncovering the truth, I say yes. But there’s nuance here. Let’s say for example (just for example, I’m not making any major factual statements here) we can treat seizures through chemogenetic intervention. Wow, that means we have a cure for seizures, right? Well… no.
Chemogenetic alterations in animal models are extremely invasive, extremely stressful, and there’s always a risk of death like with any major surgery, and in this case… we’re talking major brain surgery. So, would it be ethical to give someone suffering from seizures an invasive brain surgery that might treat some of the seizure’s symptoms? Well… I’m not so sure. There’s a philosophical argument there, right? How severe are the seizures? Might they lead to more permanent damage if they continue? How long will the genetic change brought on by chemogenetic intervention last? Will they need regular doses of something like CNO? How difficult will that make day-to-day functioning? How does the patient feel about this? These are important questions. People often talk about how healthcare should be between you and your doctor. I agree. But I also think there’s an important question here: When do we as researchers go too far with a treatment?
Now, let’s make one thing clear: I am not aware of anyone who is attempting to utilize chemogenetics to treat human illnesses, disorders, or disabilities, BUT if they were… I’d question if they were pushing the right thing, because while yes it is between the individual and their doctor, the doctor in this case would need to do what’s best for their patient, and I don’t think a dangerous, invasive brain surgery in which you inject viral loads of DREADDS into a human’s brain may be the best first option. Every surgery comes with risks - that’s certainly true - but surgeries on your brain tend to have more risks than many other much less invasive ones. We could change a lot of different mental illnesses, neurodevelopmental disorders, and more with this technology but we can’t guarantee permanence, safety, or a return to some mythical normal that doesn’t entirely exist. We also can’t target everything. Notice I used the word “Change” there rather than “cure”. I don’t think we’re curing anything. We’d just be changing a core part about how part of the brain would work. Is that a treatment? Potentially. But is the level of risk for such a treatment worth it? and would we even want to?
We can target some things. Because the brain is not one single thing, but a collection of tissue all performing different unique tasks. I couldn’t help you with hearing deficits AND help with your anxiety with the same surgery without doing multiple injections, and multiple treatments, and each time we continue to do this, risk gets higher and higher. This isn’t a cosmetic change, we’re talking about altering an individual’s brain chemistry. We can acknowledge the significance of this for research while also understanding this is something that may be better off in the research field and not expanding into actual health care. Plenty of other things do. But just for the fun of it, let’s look at a couple more examples.
Now let’s think of something less severe, but that can co-occur with seizures. Autism. Bare with me, I research Autism for a living, so it is sort of my wheelhouse, and it is the thing I have experience using viral injections in the brain for. When we inject into mice, it can help us learn a lot, but is it a treatment? Absolutely not. What exactly is Autism? Well, at its core, Autism is a neurodevelopmental disorder that leads to difficulties in socializing, stereotyped behaviors, strict routine-based behavior, and communication deficits. If I told you I could treat some of that with an invasive brain surgery that will change some of your behavior and the way you feel about things, would you want that? Honestly? If I were in that position I’d say absolutely not.
Let’s try something else. Depression. Depression is characterized by extended periods of lethargy, sadness, despair, and can be paired with suicidal thoughts and ideation. Such things can become dangerous and unsafe for the individual, certainly, but if someone told me ‘hey, I could make the bad thoughts go away. You just need to get this invasive operation.’ I think I’d be happy to stay with my hopeless thoughts. Certainly, I’m not the only person in the world with an opinion and I’m sure people would disagree, but… it’s up to the individual. In many cases, it would be a much better bet to try less invasive medications, therapies, a support system, coping mechanisms, and other things before we jump to an invasive therapy that will have a lifelong impact. My point here is, yeah… we could probably do this, but is it ethical? I don’t think it is ethical outside of for the sake of research purposes. Maybe one day it could be, but the technology isn’t there for it to be safe or to target individuals in a way that I think couldn’t risk long-term changes that may impact the individual self, health, or well being.
So, if I’m here to tell you the technology exists, but it shouldn’t be used for treatment, then why the hell do we even have this advanced technology? Simple. To understand. Put on your scientist hat with me. Or… goggles? Scientists wear goggles sometimes! Let’s put on our goggles - I’m actually more of a safety glasses guy - It’s not important. We’re wearing goggles now!
Okay, let’s say we have a genetic mouse model for dementia. Let’s say, hypothetically, that part of dementia is a decrease in connectivity between the hippocampus (memory region) and another region - let’s say the BNST (very important region for processing situational valence, fear, and anxiety - one of my favorite brain regions actually, absolutely love it). Mind you, this is entirely hypothetical, I’m not aware of any specific research on this, but we’re just using a hypothetical example.
So the hippocampus and the BNST appear to not be properly connected. Maybe they’re hypoconnected (I.e. there is a decrease in synapses connecting the two regions together compared to the average brain). Well, we could try and determine if a specific behavior can be attributed to this change in connectivity by genetically altering the number of receptors in the BNST to hopefully increase connectivity between these two regions.
This could tell us if this circuit disruption is connected to this behavioral change, and that can be a game changer! We can use that information to identify what regions are being impacted in a specific situation, and not only will that help us better understand that part of the brain, but it can also help us understand what treatments will work best. It may also give us some insight into how a specific thing is impacting one part of the brain. Because, believe it or not, system-wide alterations can have region-specific impacts. Maybe we can talk about that another time.
Now, this ethics talk isn’t to pour cold water on your sci-fi dreams, but rather to bring the point home that sometimes things like this may sound like a treatment, but I think in our very real, non-fiction world, they can and will do more harm than good if we’re not careful. But that doesn’t have to stop our sci-fi ideas from flowing. In fact, I think this is exactly where science fiction thrives. In that ethical boundary. Let’s talk more about it.
The Fiction
So, ethics aside - or exactly in front of us - what does this have to do with fiction? Well, at the top of the ethics section, I quoted Jurassic Park. And that quote is important here, because it gets into something really important. Just because we shouldn’t do it in the real world, doesn’t mean we can’t speculate about what might happen if we did it in our fiction.
Sci-fi has earned its throne as the place where shotty ethics meets science. I’m of the opinion that that is exactly where it should stay, because true science should always be as ethical and humane as possible. In our sci-fi we can reflect on why that’s so important.
If you haven’t read The Evening and the Morning and the Night by Octavia Butler, I highly recommend it. Butler delves into this idea of a genetically inherited illness caused by a cancer cure that led to unforeseen genetic changes. These changes lead to the offspring of the cancer survivors to become unstable in adulthood and literally tear themselves and others apart. There’s a terrifyingly prescient discussion about eugenics forcing its way into the story the entire time - and it is a stressful but thought provoking angle of the story - but the thing I want to focus on is the treatment. There’s this constant push and pull throughout the story about what you do with people who are ticking time bombs with the timer hidden, but it’s rare that anyone really speaks to them about it. Even though the narrator of the story is one such person, these people almost feel like passengers in their own story. Instead, they’re expected to either be hospitalized for the rest of their lives once they break from reality, or they’re expected to die.
It’s grim. Really grim. But a part of the story is the individual people who are afflicted with this disorder discovering a different path that they can help each other with. I’m not sure if it’s intentional, but it has an air of empowerment to it that I sort of enjoy. What can I say, Butler’s the Queen of Sci-Fi for a reason.
My point in bringing this up, is she takes a novel approach to treatment of a mental health condition that is centered on those afflicted. It’s really hard to center that in your story, but it isn’t impossible. So my question is: How would the individual feel when put in front of a ‘miracle cure’?
When we look at an experimental method like chemogenetics, there are endless possibilities for using it to augment super soldiers, or create unfeeling, always calculating robot-like humans, but I personally am interested in the perception of the person faced with this unethical approach and how they would react. I also think that’s important from a humanizing perspective, because we’re not talking about a mouse. We’re talking about ‘what if this happened to a human?’ and that’s worth thinking about and exploring.
So, what can we do with chemogenetics? We could create a hyperaggressive security guard protecting a cyberpunk celebrity, maybe.
Or, we could create an individual who suffers with a trauma so deep, they decide to disconnect from who they once were by disconnecting from their memories - imagine the fall out of that… feels almost like Disco Elysium which I totally didn’t play for the first time a couple months ago.
Or what about if someone was constantly hearing the voice of some other worldly being. They decide to undergo an invasive surgery to stop the voices only to discover that they’ve made the voices angrier? You could certainly go a more cosmic horror angle with this one.
There are so many ways you can take this, but… I’m not going to tell you the way I’d like to. Instead, I’ll save that for next week. You know me, I love a little suspense, so give me a week, and I’ll have a story for you! Genetic manipulation on this scale is a really amazing experimental tool, but it is just that. An experimental tool. We need to keep that in mind in reality, but when we delve into the world of fictions, why can’t we imagine a less ethical place where strange things happen and we learn why we shouldn’t by speculating on if we did.
I hope you enjoyed this new Sci-Fi Today and hopefully learned a thing or two about some fun neuroscience methodology! And maybe - if I did my job right - found a little creative inspiration along the way!
Oh, and of course! Have a look at my sources:
https://pmc.ncbi.nlm.nih.gov/articles/PMC5843707/#bph14146-sec-0015
https://pmc.ncbi.nlm.nih.gov/articles/PMC6984397/
https://www.nature.com/articles/s41380-025-03305-5
These are all fairly approachable looks into how chemogenetics works, and one of them does a great job of explaining how chemogenetics differs from optogenetics which can make both seem a little more clear. Thank you for being here and if you have any questions, please feel free to ask and I’ll do my best to clarify!
Thanks for reading and I’ll catch you next week with a story that’s been rattling around in my head. Light Show.
What a fascinating article! I have so many questions and tangents I want to ask about. Apologies in advance.
Have you read Scalzi's Lock In series? I ask because of your focus on Autism. I understand that these are different things, but the most severe cases of Autism seem to share traits of the disease in Scalzi's book. I ask because I'm curious about your take on the series.
Switching to non-fiction. Have you read Jeff Hawkins' book A Thousand Brains: A New Theory of Intelligence? The basic premise of the book/theory is that many parts of the cortex are running partial models in parallel. So the different parts of the cortex kind of 'vote' as a way to settle into agreement and create these map-like frames of reference that allows us to understand the world around us. This *could* have implications for how we build AI in that it may affect the strategies used by people like Demis Hassabis or Yann LeCun in how they build world models for AIs... if the industry ever switches from LLMs.
Back to fiction. Have you read David Brin's Uplift series? As a scientist what's your ethical take on the concept of raising the intelligence of various animals or species? Is it a good thing or a bad thing?
What are your thoughts about studies done by Cortical Labs where they have cultivated lab-grown neurons as a substrate on a microchip and then had those neurons play games: Pong and Doom. Is this proof of concept for a future of biological computing?
Well, answering any of my questions will probably involve a mini-essay. So, I'll stop machine-gunning questions at you. Thanks for taking the time to introduce me to chemogenetics. It really is an interesting concept.